PM&DC Undertaking Format for Doctors
PM&DC Undertaking Format
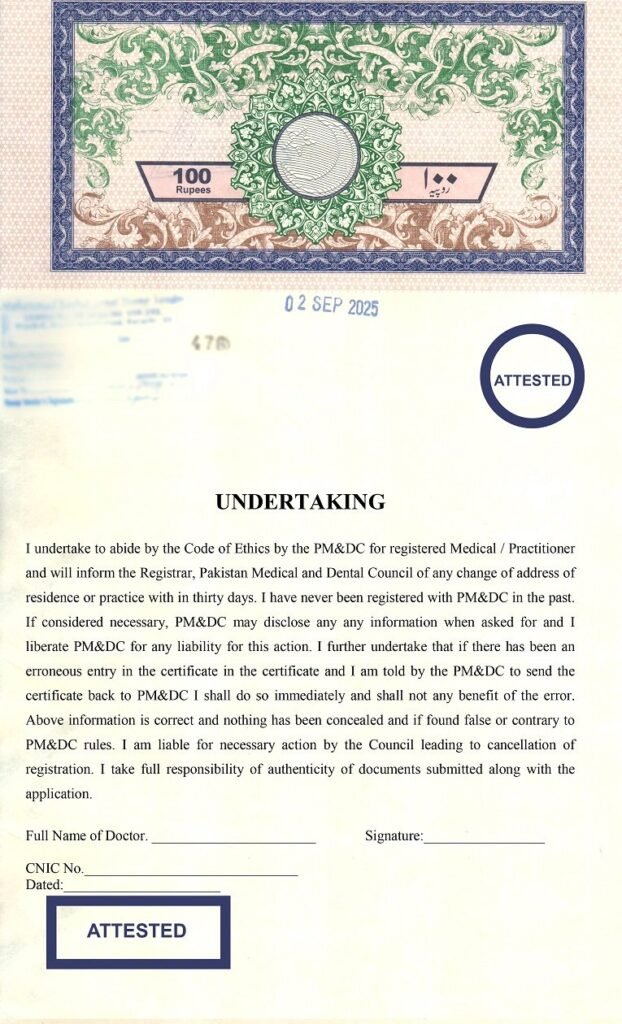
UNDERTAKING
I undertake to abide by the Code of Ethics by the PM&DC for registered Medical / Practitioner and will inform the Registrar, Pakistan Medical and Dental Council of any change of address of residence or practice with in thirty days. I have never been registered with PM&DC in the past. If considered necessary, PM&DC may disclose any any information when asked for and I liberate PM&DC for any liability for this action. I further undertake that if there has been an erroneous entry in the certificate in the certificate and I am told by the PM&DC to send the certificate back to PM&DC I shall do so immediately and shall not any benefit of the error. Above information is correct and nothing has been concealed and if found false or contrary to PM&DC rules. I am liable for necessary action by the Council leading to cancellation of registration. I take full responsibility of authenticity of documents submitted along with the application.
| Full Name of Doctor. _______________________
CNIC No.______________________________ Dated:______________________
| Signature:_________________
|
Download Pdf File : PM&DC Undertaking Format for Doctors




